



Why Did Doctors Stop Making House Calls?

There was a time when seeing the doctor didn’t mean sitting in a crowded waiting room or logging in to a patient portal. Instead, the doctor came to you, carrying a black bag and bringing their expertise and equipment to your bedside.
Today, health care looks very different. We drive to medical campuses filled with imaging suites and labs, check in electronically, and have our patient notes transcribed by AI. The transformation has been so complete that it can be hard to imagine the house call was a central feature of American medicine little more than a century ago. So what changed?

When House Calls Were the Norm
From the earliest days of American medicine through the early 20th century, house calls were a routine part of medical care in the United States. Physicians regularly traveled to patients’ homes in cities and rural areas alike. In 1930, approximately 40% of physician visits were house calls, according to the New England Journal of Medicine.
Most doctors were general practitioners who worked with patients of all ages. They delivered babies, set fractures, drained infections, treated pneumonia and influenza, and managed chronic illnesses. Medications were often dispensed directly from the physician’s bag. Payment could be made in cash or, particularly in rural areas, in goods or services.
Doctors did maintain offices, but they were often modest — sometimes located in the physician’s home — and equipped with limited diagnostic tools. Hospitals existed, but they were typically reserved for surgery, serious trauma, or advanced illness. Much everyday medical care happened in the home.
You may also like



More from our network





The Midcentury Shift
The decline of house calls was gradual at first and then dramatic. By 1950, house calls accounted for roughly 10% of physician visits; by 1980, they made up less than 1%.
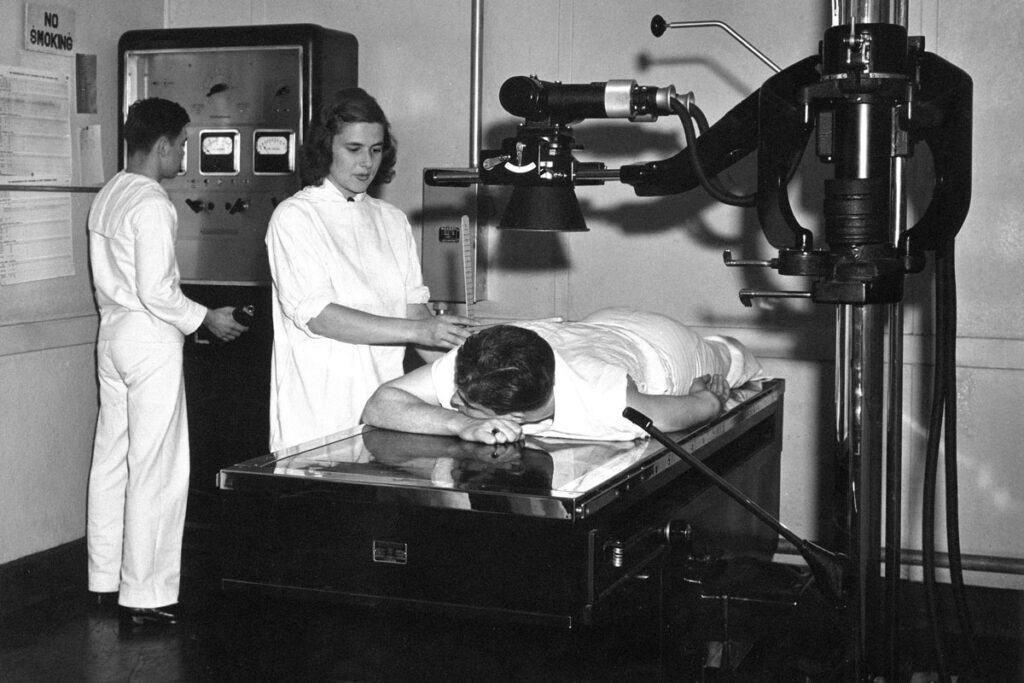
Several forces drove this change. First was the rapid expansion of medical technology in the 20th century. X-rays, laboratory diagnostics, safer anesthesia, blood banking, antibiotics such as penicillin, and eventually intensive care units transformed medicine. These advances required equipment, sterile environments, and trained support staff that could not be replicated in private homes. Hospitals became safer and more effective, particularly after improvements in antiseptic technique and infection control.
Second, medicine became increasingly specialized beginning in the late 19th and early 20th centuries. Rather than one physician handling nearly every complaint, patients began seeing cardiologists, obstetricians, surgeons, and other specialists who relied on centralized offices and hospital facilities. As care grew more complex, the home visit became less practical.

Follow the Money
Alongside advances in medical technology, economics played a decisive role in the decline of house calls. Even before the mid-20th century, home visits were time-consuming. A physician might see only a handful of patients in an afternoon of travel, compared with many more in a centralized office setting. As automobile ownership expanded and suburbs spread outward after World War II, the distances between patients grew, making travel even less efficient. Office-based care allowed physicians to treat more people in less time.
World War II intensified these pressures. An estimated one-third of American physicians entered military service during the war, creating shortages in many civilian communities. With fewer doctors available, maximizing efficiency became essential. Centralized offices and hospital-based care enabled the remaining physicians to manage larger patient loads, making routine house calls even more impractical.
At the same time, the structure of payment was changing. The growth of private health insurance in the 1930s and 1940s — followed by the establishment of Medicare and Medicaid in 1965 — formalized billing systems. Office visits were easier to standardize, document, and reimburse consistently. Home visits required travel time and longer appointments, yet reimbursement did not always reflect those additional costs, making them less financially sustainable.
Meanwhile, group practices and multi-physician clinics became increasingly common in the postwar decades. Shared equipment, centralized staff, and predictable scheduling improved productivity and stabilized revenue for doctors.

The Times They Are A-Changin’
Social change similarly played a role in the decline of house calls. As more families owned cars, traveling to a physician’s office became feasible for many folks who once relied on home visits. Urbanization, improved road systems, and expanded hospital networks also reduced geographic isolation.
Home births illustrate the broader trend. In 1900, nearly all U.S. births took place outside of hospitals, attended by either a doctor or midwife. That rate fell to 44% by 1940 and just 1% by 1969, reflecting growing confidence in hospital-based obstetric care, anesthesia, and neonatal medicine. As childbirth shifted to hospitals, one of the most common reasons for physician house calls largely disappeared.
Concerns about safety and liability also influenced practice patterns. Controlled clinical environments allowed for better infection control and standardized procedures. As medicine professionalized and regulatory standards expanded during the 20th century, office- and hospital-based care became the default model.
By the 1980s, traditional house calls had largely vanished — but they have not disappeared entirely. Geriatric and palliative care programs now provide in-home services for elderly or homebound patients. And research from the Department of Veterans Affairs and other programs has shown that home-based primary care for patients with complex chronic conditions can reduce hospitalizations and lower overall health care costs while maintaining high patient satisfaction. Telehealth has also created a new version of the house call. During the COVID-19 pandemic, virtual visits expanded dramatically after regulatory barriers were temporarily eased. While telemedicine has declined from its 2020 peak, it remains a routine part of care in many health systems.




